“Please find attached your assessment report. As we have discussed, the report is written in a diagnostic format, focusing on aspects of you as opposed to the whole of you and your life story thus far”, stated the follow up email, from the follow up appointment, from the clinician who was part of the multidisciplinary team that assessed me for autism….
It was many years ago that I attended my assessment follow up, but I still recall the nauseating anxiety as the ‘big reveal’ day approached. I knew I was autistic, my child was autistic and I’m so like them, I HAD to be autistic surely? But what if they got it wrong? What if my gender, my past psychiatric history, those traumatising life events I’d experienced, got in the way and overshadowed my innate neurology?
My follow up appointment confirmed a diagnosis of autism (level 2). Additional sensory processing difficulties were also noted, along with my past history of anxiety, depression and trauma. The report gave the opinion that some of my previous psychiatric labels were likely to be misdiagnoses and argued that some of my mental health symptoms might be better understood in the context of autism and sensory processing differences.
So how did it feel to finally get this diagnosis of autism? In fact it was the 22nd diagnosis I’d received that is listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Well, I felt ‘kind of something’ that I couldn’t quite describe – but this is normal for me, my autistic interoceptive experiences are often difficult to locate, label and explain. (Interoception is our sense system that picks up and processes body signals including pain, emotions, tiredness, hunger etc etc. Like our other sense systems, autistic people often experience sensory input differently – input may be heightened or muted, distorted, fragmented, delayed, synaesthetic, or otherwise different to that of people who are not autistic.)

Other newly diagnosed people express a whole range of human emotions when first diagnosed, including feeling nothing at all; feeling something intense; feeling validated, vindicated, relieved, terrified, angry, scared, joyful; or a few or all of these emotions; or something else entirely. Each person’s experience will be as unique as they are. There is no “right way” to feel or process the information that you are autistic.
I just received an autism diagnosis, so why do I feel bad?
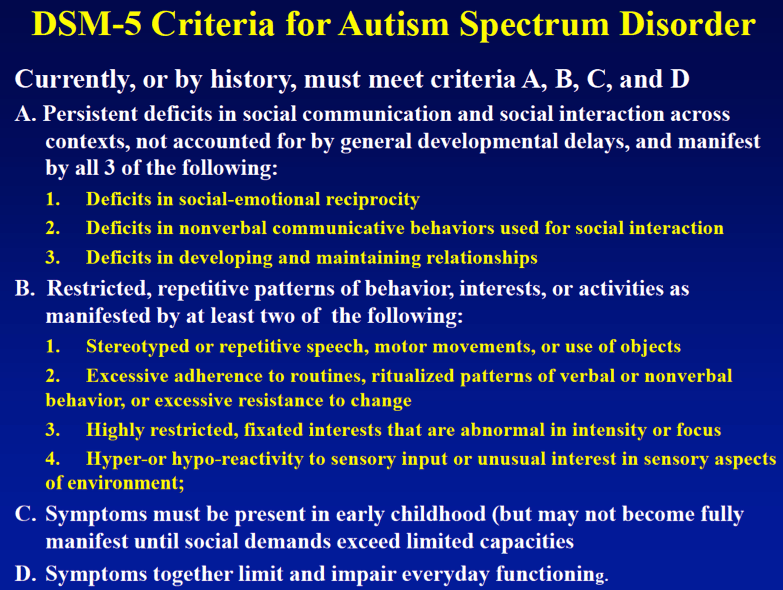
Whilst a diagnosis of autism may be validating and a relief, it can feel painful to listen to or read a list of what you find difficult. Afterall, the diagnostic criteria is largely a list of deficits – medics don’t diagnose conditions based on an individual’s strengths!
It may hurt deeply to hear loved ones describe you in ways that feel derogatory or that misunderstand your motives. An assessment report or feedback from a clinical team may feel harsh and intense and I recall feeling ashamed of how much I struggle and how often (I perceive) I have ‘failed’. My assessment report sets out my challenges in black and white – unequivocal, harsh, embarrassing, dispiriting. My report states: “Emma manages daily life exceptionally well despite her impairments, she works hard to compensate for her difficulties which prevent them being even more significant than they are.” It felt good to read that my efforts were recognised – virtually all autistic people I have met and worked with, put in huge amounts of effort to get by and survive in a world that so often feels alien and hostile towards our neurotype. I amaze myself that I can keep going sometimes!
It was important to recognise that my assessment report was a synopsis of how I met the diagnostic criteria for autism. My achievements weren’t relevant. My efforts weren’t relevant. My exhaustion from doing my best wasn’t relevant. I have written more about the diagnostic criteria in other blogs . I like to think about my autism assessment like I do the car driving test – an artificial situation that you hope to do only once; that is largely dependent on your performance on the day, that scrutinises only specific areas, and is largely irrelevant to how you actually drive the rest of the time.
On receiving my typed report, I immediately noted a few (minor) inaccuracies that screamed from the pages. I recognise now that I was a simply one human, being assessed by other humans, and the assessor’s interpretation of situations I’d described was as affected by their biases as I am by my biases. It felt difficult though, when reading certain aspects of the report which led to those all-familiar feelings of being misunderstood. Of course, my eagle eyes were working at their sharpest when reading my report, on account of the expectation and anxiety that sharpens your senses and increases your vigilance when under threat – in fact, like all animals in a survival situation, I was tuned in to perceived threats and unable to pick up on cues of safety – and don’t think any typos escaped my keen observation! I’d recommend to anyone receiving the outcome of their assessment, to structure your time in the subsequent days so that you can do whatever self-care works for you and that will help with processing all the information. I have written about autistic self-care in other blogs.
Several years later, I can read my assessment report and feel very little. It doesn’t trigger me, and I have had time to process its contents in my own way. Processing, as the name suggests, is a process! I have thought and felt a variety of things about my diagnosis over the years, and no doubt will continue to do so.
Why did my new diagnosis of autism feel so good?
Quite simply, because I felt seen for who I am. For me, a person with multiple psychiatric diagnoses, some accurate, some questionable, my autism diagnosis explained how I experience the world and offered me a lens through which to revisit every life experience I’d had. My diagnosis made sense. It felt right – and as someone who likes things to be accurate, this was hugely important. My previous diagnoses had never felt 100% right. Sure, some of them resonated – anxiety and depression, for instance – they explained ‘what’ was going on, but not ‘why’ I kept finding myself in the midst of them. Other past psychiatric diagnoses seemed completely off target and almost the opposite of my lived experience. My autism diagnosis meant I felt validated. I almost felt like shouting to the world, “see, this is why I find everything so bloody difficult!”
Now that the outcome is sinking in:
It is normal to think and feel differently about your diagnosis as time moves on. Some people may never feel anything significant about their diagnosis. Other people may wish for the diagnosis to be taken away. Expectations about future support and understanding following diagnosis may be realised – or sadly as is so often the case, there is little support out there unless you are in crisis.
Here are some questions and scenarios that newly diagnosed people may ask or share, and some responses (responses are based on my personal and professional experience and are not recommendations).
Should I tell my family/my school/my workplace?
It’s up to you! Some people feel a need to tell the world they are autistic but there is no obligation to. You may choose to tell no-one. You may decide to share your diagnosis on a case by case basis. You might decide to blog about it and tell the world, like I did!
I’ve been told by friends/family/colleagues that I don’t seem autistic…
This is unsurprising in some ways because often people only learn about autism through the media and stereotypes. People may be comparing you to the only other autistic person they know e.g. a friend’s child. They may be unaware of how much time you spend masking in order to stay safe. There is no right way to respond to this situation and it might help to join online communities or find local peer support groups to discuss this with. I find that often people say this as a compliment, they are trying to be kind – but of course, it doesn’t feel like a compliment and can be invalidating. Whether you challenge people on this or not is up to you. I rarely do, but I am in quite a privileged position where I am usually taken seriously.
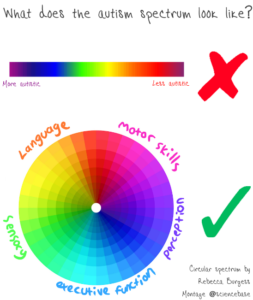
Aren’t we all on the spectrum?
No. You may like to read this earlier blog or recommend it to people. Autistic experiences are human experiences. Most people understand what it is like to be so overwhelmed by your surroundings you can’t think straight; or to have your anxiety reduced by carefully planning your day; or understand the joy in hearing a tune so beautiful you can’t help but move. When we shift our thinking from “aren’t we all a bit autistic?” to “no, but we are all human” it can prompt us to recognise the inequalities autistic people face and question why some people experience distress and difficulty so much of the time compared to their non-autistic peers.

Here are three examples of common human experiences that autistic people may experience more frequently and more intensely due to the world not offering enough opportunities for inclusion:
1. It’s too noisy to think straight.
Autistic people may need to wear noise cancelling headphones or ear defenders to cope with everyday background noise, because our brains may not filter sound. It can feel overwhelming and panicky and we may be unable to focus on, or even work out what is important. Non-autistic people may recognise these types of feelings when trying to park their car when it’s raining heavily, the kids are chatting in the back of the car and the radio is on loud. Typically, they may ask the kids to be quiet or turn down the radio so they can find a parking space. (Note that a reduction in auditory input, frees up visual processing capacity. Our sense systems work together and noise cancelling headphones/ear defenders may be useful for reducing sensory input in many situations, not just ones perceived as noisy) It may help understand me better if you consider that my “normal” when it comes to noise, is like your “parking in the rain with the kids screaming and the radio blaring”.
2. You look like you’re over-reacting.

All humans find that our sense sharpen when we are anxious. Autistic people’s senses may often be sharpened on account of our different neurology. A survival response of fight/flight/freeze is not a choice, but proportionate to what our brains perceive. It certainly isn’t an over-reaction. If we are home alone at night feeling anxious and suddenly hear an unexpected noise in the house, it is likely to cause us to jump and may seem louder than the same noise during the daytime when we are busying about and there is an abundance of background noise.
3. A change of plan feels the last straw.
Most of us can relate to feeling deeply disappointed at a change of plan. Again, we need to consider proportionate responses. If I am distressed because you are five minutes late, it is not an overreaction and may be because to me, five minutes feels like 20 minutes does to you (I like to think the ‘sense of time’ is a human sense system too, maybe we could name it chronoception?). Maybe it’s because my imagination knows no bounds and I can think up infinite reasons why you may be late, but have no gut feeling about which of those reasons may be accurate. Once you are a few seconds late, I have no way of knowing when you may come and how this might impact our plans and the rest of my day – and planning my day is important because it provides some predictability to an otherwise chaotic experience. You’d probably be distressed if your holiday of a lifetime was cancelled. I may value my hobbies and interests as highly as you value your holiday, and feel just as distressed if my plans were changed.
Will I get more support at work/school now?
Perhaps. Not every school or workplace is equal in terms of reasonable adjustments and support that may be offered. Legislation is in place to ensure disabled people are not discriminated against but we know the reality is that often employers and educators feel helpless in terms of their understanding of autism and how to best support people. There are organisations that specifically support people in education and employment, they may be able to offer bespoke or more general support.
Why have I suddenly become more autistic?
It seems quite common for newly diagnosed people to embrace their diagnosis and reduce some of the conscious masking they have done. Those self-soothing habits I used to suppress, like rocking from side to side when waiting in a queue, felt permitted once I was formally told I was autistic. None of those “more autistic” things were fake or put on, I felt validated and “allowed” to be more authentic. I accessed a newfound confidence and was able to be more myself. Other people may have perceived this as me playing on my diagnosis, or they may have attributed some other motive to what they perceived as my out of character or exaggerated behaviour. I do recall appearing “more autistic” at first after my diagnosis, but it has settled now. This book was useful to me and I’ve recommended it to others.
It’s not fair. I’ve been bullied, misunderstood and treated badly, simply for being myself.
Correct – it’s not fair, and this may feel doubly harsh because autistic people so frequently call out injustices. Fairness seems important to many autistic people. I have been working on cultivating compassion and self-compassion. It’s not easy when your life has been full of mistreatment and a continuous stream of micro-invalidations. (I use the word micro-invalidation to mean those comments that usually start with “no-one else is…” and end with something related to our way of experiencing the world e.g. “complaining about the food/lights/noise/moving about/not paying attention/forgetting their book”).
I’d like to say that I don’t dwell on the negatives, but with a brain that can hyperfocus, seek solutions to problems, and ruminate on injustices with the strength of superglue, it is not easy to unstick these type of thoughts. Many of us could have felt intense shame for how we are, we may have internalised stereotypes and negative ideas about autism and find self-compassion is an alien concept. As I’ve processed my diagnosis, re-evaluated my life through the lens of autism, and got to know myself more deeply, I feel more at peace. Again, it is a process.
I’ve moved through experiencing validation and relief, to finding disappointment that the world is still as tough as ever post-diagnosis. I’ve felt proud to be autistic, embarrassed to be autistic. I’ve chosen to mask my autism when it’s less costly than being open about it. I’ve felt angry at the bullies, angry at the medics who repeatedly got it wrong, angry at society for having an accepted culture of mocking differences. Writing helps me process things, so I’ve written lots. I am bringing up my child to be unashamedly themselves.
What can I do to make life easier?
It can be a harsh realisation when you recognise that the world continues to be a challenging place to exist. Here is a non-definitive list of ten things that may make life easier:
- Play to your strengths and use your need for routine, your ability to hyperfocus, your incredible eye for detail, or whatever your strengths may be to have a fun and fulfilling life.
- Don’t feel you have to tell anyone you are autistic unless you choose to.
- Don’t feel you have to hide you are autistic either.
- Explore your sensory profile. Those sensations you seek out or avoid. Plan regulating sensory experiences into your day. These are experiences that help you feel balanced and at your best. I find walking, stretching, using headphones, stroking soft material, crunching crisps, all help me be regulated.
- Consider creating a one-page document that lists how others can help you best. You may like to share it with work/school, hospital staff, group leaders etc. If you are stuck for ideas, leave a comment and I’ll share some examples you might like to adapt.
- Be proactive with your self-care and self-regulation.
- Read, watch and learn about autism from other autistic people.
- Be kind to yourself. This can be tough if you’ve felt there was something wrong with you prior to realising you’re autistic.
- Find out about reasonable adjustments at school and work and consider what may help you. Internet searches will bring up many organisations that have free resources. Here’s a link to an employment event where I delivered a workshop for the National Autism Team in Wales.
- You don’t require a formal diagnostic assessment and diagnosis to be autistic. Afterall, you were autistic before you got your diagnosis. Assessment is not available to everyone, for a variety of reasons, or you may simply choose not to pursue a diagnosis by this route.